
3/25/26
Women’s Health Gets Federal Attention
Insights from the inaugural Health and Human Services National Conference on Women's Health in Washington, DC.

Back to Resources



Summary
The inaugural HHS National Conference on Women's Health surfaced systemic gaps in maternal care, perimenopause and menopause treatment, and chronic disease management for women. Despite spending over $20,000 per birth, the U.S. has the worst maternal outcomes of any high-income country, and more than 80% of pregnancy-related deaths are preventable. Speakers highlighted federal momentum, including CMS's Transforming Maternal Health (TMaH) Model and the FDA's November 2025 removal of the black box warning on hormone therapy. Mental health was woven into every discussion, signaling a shift toward whole-person care for women across the lifespan.
“Women’s health is one of the great underserved areas of healthcare.”
Kate Ryder, founder and CEO of Maven Clinic, said it plainly from the stage. It landed less like a provocation and more like a fact everyone in the room already knew, nodding their heads enthusiastically in agreement.
That was the throughline at the inaugural National Conference on Women’s Health, hosted by the U.S. Department of Health and Human Services: less introduction than reckoning, less abstract ambition than long overdue course correction.
The program reflected the priorities of the current federal administration, while also surfacing conversations about lived experience, research, diagnosis, treatment, education, and cross-sector innovation across the lifespan. Mental health was woven into nearly every discussion: spanning perimenopause and menopause, maternal health, chronic disease, data infrastructure, care delivery, even private-sector innovation. Panelists repeatedly made clear just how much of women’s health research has been underfunded, women’s clinical care understudied, and many women in need of care left feeling misunderstood – and what the current federal administration says it will do about it.
Maternal health crisis front and center
The problem was laid bare in maternal health. Speakers described a system with poor outcomes, large access gaps, and a postpartum period that remains dangerously under-supported.
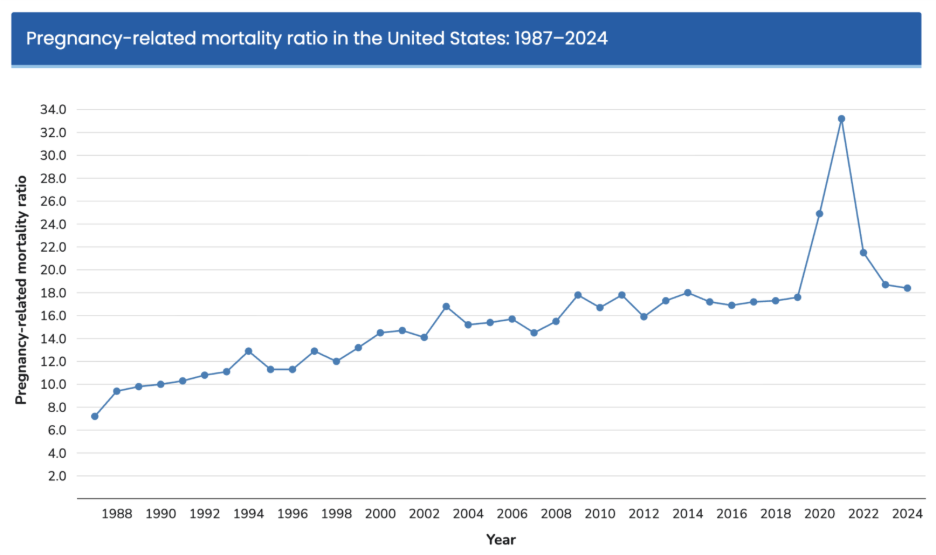
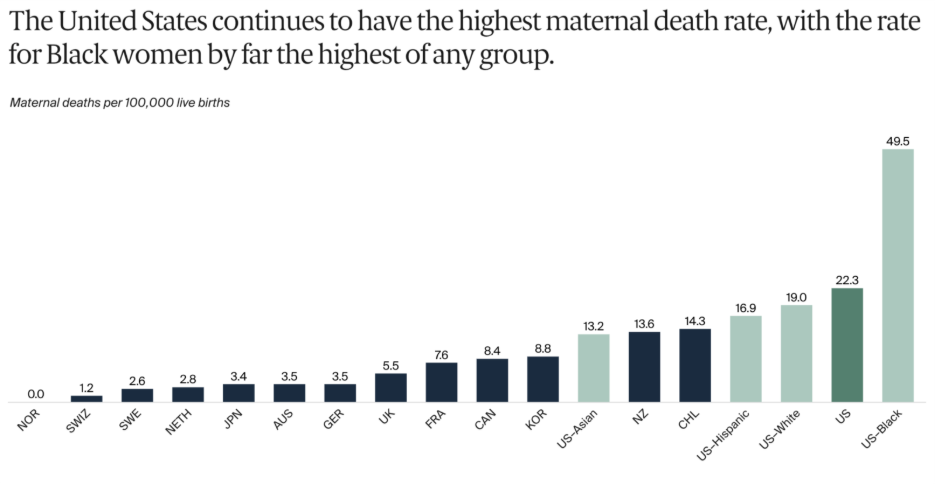
Despite spending more on pregnancy, childbirth, and post-partum care than any other high-income country (an average of over $20,000 per birth, per data analysis by Peterson-KFF) the U.S. continues to have much worse maternal health outcomes, a trend that’s been rising for decades. Maternal mortality is highest for Black women.
More than 80% of these pregnancy-related deaths are preventable – deaths that occur not just during delivery but throughout pregnancy and the full year postpartum. Meanwhile, according to a 2024 March of Dimes report, more than 35% of U.S. counties are classified as maternity care deserts, meaning no birthing hospital or obstetric clinician is available locally.
These aren’t just physical health or logistical issues for women; they’re mental health issues, too. Stress, isolation, untreated depression and anxiety, and lack of follow-up care are part of the maternal health crisis.
“We need to treat the whole mom and take a whole-person approach.”
Momentum appears to be gathering to address this crisis. With Medicaid currently covering about 40% of U.S. births, CMS is betting on broader, whole-person maternal care through its Transforming Maternal Health (TMaH) Model, now underway with 15 state Medicaid agencies to test whole-person, value-based approaches to pregnancy, childbirth, and postpartum care.
Panelists made a parallel point about care design: the best-performing maternal systems are not narrowly obstetric. They are collaborative, longitudinal, and increasingly inclusive of mental health as part of whole-person care. “We need to treat the whole mom and take a whole-person approach,” said Olivia Walton of Heartland Forward’s Maternal & Child Health Center.
An emphasis on the benefits of hormone therapy
The Women’s Health Initiative (WHI) study was surfaced over multiple sessions as a reminder of how one set of findings can shape decades of medical practice.
In 2002, the study linked hormone therapy to breast cancer, stroke, blood clots, and heart disease, scaring a generation of women away from treatment and reshaping care almost overnight.
But the story turned out to be more complicated. The study focused largely on older women, on average 10 years post-menopause, using one regimen that does not reflect how hormone therapy is typically prescribed today. The current view is far more nuanced. Research now suggests that hormone therapy can most benefit women who are in the “window of opportunity” – within 10 years of menopause (or under age 60) – and is considered a safe, effective treatment, with risk shaped by timing, formulation, and individual health history.
That recalibration is now changing policy. In November 2025, the FDA removed the black box warning statements on hormone therapy related to cardiovascular disease, breast cancer, and probable dementia. The agency’s updated language reflects a more current view of benefit-risk considerations, particularly for women who begin treatment closer to menopause onset. On stage, the more practical question was not whether the science has evolved, it was whether physician education will evolve with it.
Women and chronic conditions
That question kept surfacing in different forms throughout the conference. Many chronic conditions disproportionately affect women are still too often under-researched or under-diagnosed. Heart disease remains the leading cause of death for women in the United States. Nearly two-thirds of Americans living with Alzheimer’s are women. Approximately 80% of all patients with autoimmune diseases are women. And major depressive episodes are more common among adult women than men.
These are not niche issues. They are central to population health.
“Invisible illness requires visible science.”
Speakers returned, again and again, to the problem of visibility. Nicole Kleinstreuer, NIH Deputy Director, captured it in one line: “Invisible illness requires visible science.”
Jay Bhattacharya, the NIH director, put the broader stakes just as clearly: “How do we make America healthy again without making women healthy?”
By the end of the conference, the most important takeaway wasn’t a single statistic or policy announcement. It was a shift in framing. An acknowledgement that women’s health is finally being discussed as it is: interconnected. Physical health, mental health, maternal health, aging, and chronic disease all influencing and shaping one another over time.
That’s a more accurate picture of women’s lives. It’s also a more useful one.
The real test now is whether this shift changes care and improves outcomes for 51% of the population. Not just on conference stages or in federal programs, but in exam rooms, care pathways, postpartum follow-ups, menopause treatments, and the quieter moments when women are too often told their symptoms are normal, inconvenient, or all in their heads.
Seeing women's health more clearly is progress. Acting on it is what matters most.





ABOUT THE AUTHOR

Kristen Sills
Head of Marketing

Latest Articles

7/22/26
ieso Welcomes Mike Chynoweth as Head of Engineering
An engineering executive who translates strategy into execution and builds teams that deliver quality at speed, Mike Chynoweth brings over 20 years of experience across healthcare, security, and regulated SaaS to ieso as Head of Engineering.

7/8/26
Joy Isn't a Reward for Healing
Dr. Talia Cohen and Alyssa Dietz, PhD, on chronic conditions, identity, lived experience, and the mental health piece most digital health companies are still missing.

6/17/26
CBT? ACT? What’s the Difference?
CBT and ACT are closely related, but they work differently. ACT helps you create space between yourself and your thoughts, a skill that can be helpful if you're managing the stress, uncertainty, and emotional weight of living with a chronic condition.

6/4/26
ieso Welcomes James Dold as Head of Sales
A healthcare leader with clinical roots, James Dold brings over 20 years of experience across behavioral health, value-based care, strategic partnerships, and care delivery to ieso as Head of Sales.