
4/23/26
Chronic Pain Programs Are Still Treating Only Half the Patient
Most MSK and chronic pain programs are built around an incomplete model. Here's what the behavioral layer they're missing is costing them — in outcomes, engagement, and ROI.

Back to Resources



Summary
Digital MSK and chronic pain programs that skip the behavioral layer lose members in the hardest stretch of recovery. Nearly 25% of U.S. adults live with chronic pain, and MSK conditions drive over $300 billion in annual medical spending. Research shows 39.3% of chronic pain patients have clinical depression and 40.2% have anxiety, with fear-avoidance, catastrophizing, and low mood driving disengagement and worse outcomes. Cognitive behavioral therapy and acceptance and commitment therapy improve pain-related function and adherence. Integrated behavioral support is what keeps members in care long enough for outcomes and ROI to materialize.
At the VA, I ran group therapy for veterans living with chronic pain. I can still see one man clearly. He couldn't sit in a chair like everyone else. Instead, he knelt on the floor for the entire session because sitting was too painful.
I saw how constant pain had ravaged his body. Beneath his tired, strained face and behind his deliberate movements, I saw what it had done to his life, too.
Chronic pain makes your world feel small. It steals your sleep, robs you of joy, and hijacks your identity. It makes you cranky, irritable, and withdrawn. The veterans in my group were there because surgery had either failed them or didn't seem worth the gamble, they didn't want to rely on opioids, and cortisone injections had bought them a few weeks of relief at most. They were looking to show up for the things that mattered to them: their families, their work, their identity.
What they needed – and didn't get in physical therapy – was support for the full weight of what they were carrying.
That experience shaped how I think about chronic pain care. And it's why I think most musculoskeletal (MSK) and chronic pain programs today are still built around an incomplete model.
For the digital health companies now building these programs, that's showing up directly in outcomes and costs.
Chronic pain is one of the biggest, most expensive unsolved problems in U.S. healthcare
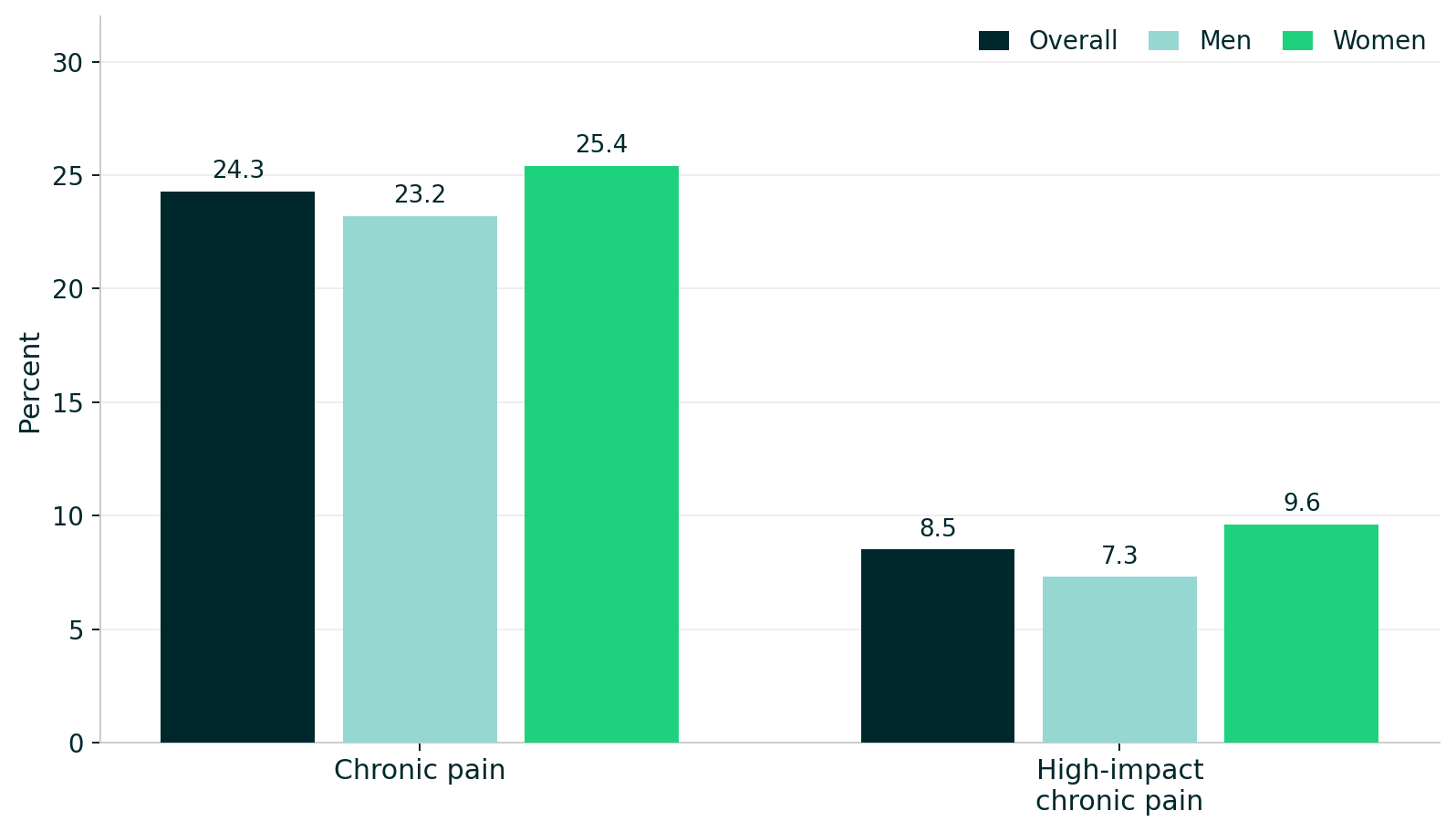
Chronic pain – including low back pain, neck pain, osteoarthritis, headaches and migraines, fibromyalgia – is one of the most prevalent and costly conditions in the U.S. Nearly a quarter of U.S. adults report chronic pain, and 8.5% have high-impact chronic pain that frequently limits life or work activities. Both affect more women than men.
It's not just a veteran's or older-adult issue. Chronic pain affects more than 12% of young adults ages 18–29 and climbs to 36% in people 65 and older.

The economic footprint is enormous. Musculoskeletal conditions account for more than $300 billion in total medical spending per year, with employers bearing a disproportionate share of those costs. Low back pain alone is the leading cause of disability in 160 countries.
And yet a lot of that spending is on interventions that don't solve the problem. Take low back pain, for instance. It's most often idiopathic – no clear structural cause – and resistant to many of the interventions payers spend the most on. Expensive surgery frequently doesn't work. Patients cycle back through the system, generating costs long after the procedure, because the underlying drivers of their pain and disability were never addressed.
This is what makes chronic pain such a high-value target for digital behavioral intervention. The opportunity isn't just to treat episodes, or even to cure the pain entirely. It's to alter the trajectory.
Poor outcomes are driven by a behavioral layer most digital programs don't treat
The connection between chronic pain and mental health is reciprocal and well-established. A 2025 meta-analysis of 376 studies and 347,468 adults found clinically significant depression in 39.3% of people with chronic pain and anxiety in 40.2%. A separate 2024 prospective study found consistent bidirectional associations between depressive symptoms and chronic pain in middle-aged and older adults.
Practically, this means that chronic pain can drive depression, anxiety, hypervigilance, and fear. Those mental health states in turn make pain harder to regulate, more disabling, and less responsive to treatment. For instance:
- Fear-Avoidance Model – beliefs that movement will make pain worse keep people sedentary and physically deconditioned.
- Catastrophizing – assuming the worst-case scenario – amplifies pain intensity and increases disability.
- Depression and low mood reduce motivation and disrupts the consistency that rehabilitation and PT require.
- Sleep disruption, driven by anxiety and rumination, worsens pain sensitivity.
Research shows that fear-avoidance beliefs and depression are consistent predictors of worse pain outcomes – not because they cause the pain, but because they determine how people respond to it and whether they stay engaged with care.

The goal in chronic pain isn't to eliminate pain entirely. That's not a realistic target for most people. The goal is to reduce pain interference: what pain does to a person's capacity to work, move, sleep, and stay in care.
As I frame it clinically: we're not going to remove the pain completely, but we can help reduce the intensity of the experience of pain.
Why digital MSK programs lose members before they deliver ROI
Digital chronic pain and MSK programs face a specific attrition problem. Members enroll with high expectations, but as soon as they hit a difficult stretch – a flare-up, a week of poor sleep, a session that felt harder than expected – they disengage. The physical therapy protocol may be evidence-based, but if the behavioral layer isn't addressed, members don't have the tools to tolerate the hard parts of recovery. They interpret difficulty as failure. So, they stop.
This is the "boom-bust" cycle in practice: someone pushes hard on a good day, overdoes it, pays for it physically, and retreats. Without support that helps them understand how to pace themselves and stay connected to why they enrolled in the first place, disengagement is almost inevitable. And disengaged members don't generate outcomes data, renew, or demonstrate ROI.
A Mental Health America analysis of over 160,000 people with chronic pain found that 79% screened positive for a mental health condition, yet 36% had never received any mental health treatment or support. These people want help, but there are so many barriers in their way: fragmented care, discomfort disclosing new symptoms, and no clear pathway to get mental health support inside the program they're already using.
Integrated behavioral support changes adherence, outcomes, and cost
The evidence is substantive. A 2025 randomized clinical trial found that both mindfulness-based therapy and Cognitive Behavioral Therapy (CBT) improved pain-related symptoms and function, and reduced opioid dose, through 12 months in adults with chronic low back pain. A 2024 review found that Acceptance and Commitment Therapy (ACT)-based approaches improve pain-related functioning and psychological outcomes across chronic pain populations. These approaches work because they target the mechanisms that often determine whether someone stays in care: fear, catastrophizing, and avoidance, not just whether pain scores shift.
When behavioral support is embedded into a chronic pain program, members are better able to tolerate flare-ups without spiraling. They pace themselves instead of swinging between overdoing it and shutting down. They find ways to stay connected to what makes them feel whole, even if that means accepting life looks different than it did before pain took over. That's what keeps people in care long enough for it to work.
For chronic pain and MSK platforms, this is the real test. Along with exercises, education, or even some early symptom relief, can keep people engaged through the hardest stretch of recovery, when pain spikes, sleep falls apart, and progress feels uncertain?
I learned from those veterans that chronic pain is never just about pain. It is about all that pain interrupts. What it makes people believe about themselves and their future.
The programs that recognize this, and offer support for it, will keep more members in care, generate stronger outcomes, and build a more believable ROI story. The ones that don't will keep offering help that is technically sound, but too narrow to change much.





ABOUT THE AUTHOR

Alyssa Dietz, PhD
Head of Clinical Strategy

Latest Articles

7/22/26
ieso Welcomes Mike Chynoweth as Head of Engineering
An engineering executive who translates strategy into execution and builds teams that deliver quality at speed, Mike Chynoweth brings over 20 years of experience across healthcare, security, and regulated SaaS to ieso as Head of Engineering.

7/8/26
Joy Isn't a Reward for Healing
Dr. Talia Cohen and Alyssa Dietz, PhD, on chronic conditions, identity, lived experience, and the mental health piece most digital health companies are still missing.

6/17/26
CBT? ACT? What’s the Difference?
CBT and ACT are closely related, but they work differently. ACT helps you create space between yourself and your thoughts, a skill that can be helpful if you're managing the stress, uncertainty, and emotional weight of living with a chronic condition.

6/4/26
ieso Welcomes James Dold as Head of Sales
A healthcare leader with clinical roots, James Dold brings over 20 years of experience across behavioral health, value-based care, strategic partnerships, and care delivery to ieso as Head of Sales.