
5/20/26
Digital GI Care Has an ROI Ceiling. Mental Health Is How You Break Through It.
Digital GI platforms have closed major access gaps and proven real ROI. The unaddressed mental health burden in IBS and IBD populations is capping how much further those outcomes can go.

Back to Resources



Summary
Digestive disorders cost the U.S. $112 billion a year, and mental health is a major driver. Over 38% of IBS patients have anxiety and over 27% have depression, roughly double general-population rates. In IBD, comorbid anxiety or depression is tied to a 60% higher flare risk, a 35% higher rate of hospital admissions, a 30% higher rate of ER visits, and a 63% higher rate of surgery. Digital GI programs like SonarMD, Oshi Health, and Cylinder Health have already proven strong ROI, but gains risk stalling when mental health is treated as a separate referral. Alyssa Dietz, PhD, Head of Clinical Strategy at ieso, lays out why specialized, evidence-based mental health support, especially Acceptance and Commitment Therapy, works best when it lives inside the GI care experience patients already trust.
Think about this: a majority of irritable bowel syndrome (IBS) patients say they would give up 10 to 15 years of life expectancy for an instant cure.
I came across that figure years ago, and as a clinical psychologist, it has never left me. It speaks to a reality of living with IBS that no symptom scale or quality-of-life score can quite capture.
Living with a GI condition is constant work. Before a dinner party, someone with IBS has already run through a mental checklist. Where’s the bathroom? What’s on the menu? Can I eat that? What happens if I can’t?
The physical symptoms are real: pain, bloating, urgency, unpredictability. But the mental burden shapes every social decision, every meal, every trip away from home. Over time, the mental calculus starts to win. Plans get canceled. Invitations go unanswered. The world gets a little bit smaller.
In my experience, the patients who struggle most aren’t always the ones with the worst physical symptoms. They’re the ones whose mental health has never been part of the conversation.
Here’s what it costs to leave mental health out of GI care, and what becomes possible when you layer it in.
The gut-brain axis is real, and GI conditions aren’t “all in your head”
To understand why mental health is so entangled with GI conditions, you have to start with biology. The gut and brain are in constant conversation through the nervous system, hormones, immune signals, and the microbiome. This bidirectional relationship is well-documented. Stress and anxiety can intensify GI symptoms. Severe or unpredictable symptoms can worsen anxiety, mood, and sleep.
What I see clinically is that this loop tends to feed on itself. Patients develop what I think of as the “spotlight effect”: a kind of hypervigilance where someone is constantly scanning their body for signals, which then amplifies their experience of symptoms, which fuels more anxiety, and so on. It’s exhausting, and over time, it changes how people with GI issues move through the world.
This is true regardless of which GI condition someone is living with. Inflammatory bowel disease (IBD) — most commonly Crohn’s disease and ulcerative colitis — has a clear physiological basis: chronic inflammation with autoimmune components. IBS is different. Its cause isn’t fully understood, and although current guidelines treat it as a positive symptom-based diagnosis, in practice it’s often only confirmed once other conditions have been ruled out.
But neither is “all in your head.” Both are real, are physically and psychologically taxing, and involve a brain and gut that are deeply intertwined.
Mental health is a big driver of the $112 billion annual cost of GI care in the U.S.
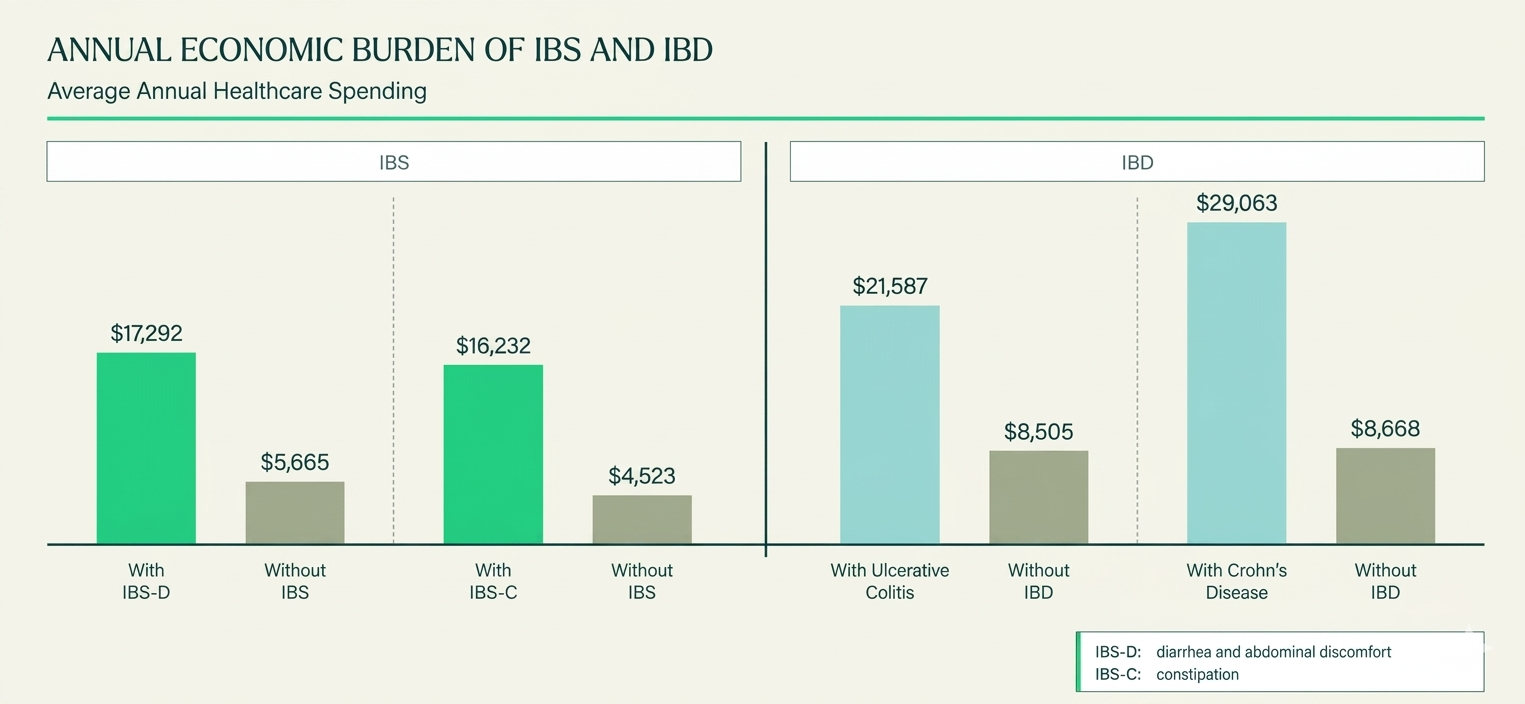
GI conditions are costly and common. According to the Peterson Health Technology Institute (PHTI), digestive disorders account for $112 billion in total annual U.S. healthcare spending.
IBS affects up to 15% of U.S. adults, with annual healthcare spending exceeding $16,500 per patient. For the nearly 1 in 100 Americans with IBD, average annual spend is around $25,000, often double that in moderate-to-severe cases.
Mental health is a significant part of why. An analysis of more than 1.2 million IBS hospitalizations found that over 38% of patients had anxiety and over 27% had depression, roughly double the rates in the general population. A large meta-analysis found roughly 32% of IBD patients experience anxiety and 25% experience depression, with rates climbing during active disease.
“Patients with psychiatric comorbidities (especially anxiety and depression) have more pain, more emergency visits, and more likelihood of presentation without active inflammation,” says Dr. Ashwin Ananthakrishnan, a gastroenterologist at Massachusetts General Hospital and Associate Professor of Medicine at Harvard Medical School.
The data bears that out. IBD patients with co-morbid anxiety or depression have a 60% higher risk of disease flare, a 35% higher rate of hospital admissions, a 30% higher rate of ER visits, and a 63% higher rate of surgery than those without.
The mental health burden isn’t separate from the cost burden. It’s a direct contributor.
Digital GI companies are already proving the ROI of better care
Digital GI companies have done extraordinary work closing access gaps in a system where gastroenterologists have the third longest specialist wait times in the U.S. and two-thirds of counties have no practicing gastroenterologist at all. Symptom tracking, nutrition guidance, care navigation, specialist access, medication management — these are meaningful clinical services that reduce the diagnostic odyssey GI patients often endure for years.
The ROI is already compelling:
- SonarMD reports 85% patient engagement, 50% fewer hospitalizations, and more than $3,000 in annual savings per patient.
- Oshi Health shows $10,292 in all-cause medical cost savings per patient in six months, with 92% of patients reporting symptom improvement.
- Cylinder Health published data showing a 5.87:1 ROI, with more than $2,000 PMPY savings against a $345 PMPY program cost.
These are real numbers driving real outcomes. And they represent only part of the opportunity. The flare risk, ER visits, hospital admissions, and surgical escalation tied to untreated anxiety and depression are exactly the cost drivers these programs already work to prevent.
Leaving mental health outside the digital care model leaves outcomes and savings on the table.
Why mental health support for patients with digestive disorders looks different than standard therapy
When I think about what actually works for GI populations, I lean toward Acceptance and Commitment Therapy (ACT) over generic CBT. The reason is specific to what living with a GI condition involves.
A major component of second wave CBT work focuses on identifying distorted thoughts and gathering evidence against them. In many contexts, that approach is highly effective. But for someone with IBS or IBD, the feared outcome — an accident, a flare in public — can and does happen. Asking someone to disprove their fear doesn’t hold up when the evidence from lived experience sometimes confirms it. That can deepen the spotlight effect rather than relieve it. (Specialized CBT protocols, like gut-directed CBT, are a meaningful exception. They’re built specifically for GI populations and avoid the pitfalls of the generic approach.)
ACT takes a different path. It builds the capacity to act in line with your values even when discomfort and uncertainty come along, too. Someone with IBS can’t always guarantee that the dinner party will go smoothly. ACT helps them go anyway, and handle whatever shows up with less shame, fear, and avoidance. Over time, that translates into something patients feel directly: a better quality of life, not just lower symptom scores on the GAD-7 or PHQ-9.
Emerging research supports this. RCTs of ACT in IBD populations have shown meaningful reductions in stress, anxiety, and depression symptoms. The approach also directly addresses avoidance, the behavioral mechanism that, when left unchecked, leads people to disengage from the activities and relationships that make life worth showing up for.
This is why GI populations need mental health support that’s clinically matched to what they’re actually facing. A generic therapy referral often misses the mark. Specialized, evidence-based care does not.
The mental health layer works best when it lives inside the GI care patients already trust
Here’s what I find most exciting about this moment in digital GI care. The infrastructure is already there. Patients trust these platforms and actually use them. The engagement metrics are the envy of mental health apps. The workflows are driving real outcomes and real savings. That’s the hard part.
So when mental health gets handled as a separate referral or a standalone app, something is lost. Patients have to start over somewhere new, with someone who doesn’t know their flare patterns, food triggers, care team, or history. In my clinical experience, most won’t. The ones who do tend to drift away within weeks. The connection between GI care and mental health support breaks at exactly the moment it should be tightest.
When evidence-based mental health support lives inside the digital GI experience patients already trust, the dynamic shifts. Engagement holds, because there’s no new login or new relationship to build from scratch. The clinical work becomes sharper, because it’s informed by what’s actually happening in someone’s GI care. And the ROI compounds, because mental health is now acting on the same outcomes you’re already accountable for: adherence, flare prevention, utilization, and total cost of care.
I’m not suggesting GI platforms become mental health companies. I’m saying the engagement, trust, and outcomes already built into these platforms can work harder when you address one of the most powerful clinical drivers hiding inside your population.
Digital GI care has proven it can reduce the burden of digestive disease. The next step is making that care complete.
Learn more about Velora, ieso’s evidence-based digital mental health program built for chronic condition care.





ABOUT THE AUTHOR

Alyssa Dietz, PhD
Head of Clinical Strategy

Latest Articles

7/8/26
Joy Isn't a Reward for Healing
Dr. Talia Cohen and Alyssa Dietz, PhD, on chronic conditions, identity, lived experience, and the mental health piece most digital health companies are still missing.

6/17/26
CBT? ACT? What’s the Difference?
CBT and ACT are closely related, but they work differently. ACT helps you create space between yourself and your thoughts, a skill that can be helpful if you're managing the stress, uncertainty, and emotional weight of living with a chronic condition.

6/4/26
ieso Welcomes James Dold as Head of Sales
A healthcare leader with clinical roots, James Dold brings over 20 years of experience across behavioral health, value-based care, strategic partnerships, and care delivery to ieso as Head of Sales.

6/1/26
Mental Health Isn’t Separate From Women’s Health - So Why Is It Still Treated That Way?
As women’s health companies expand care services, mental health can't sit on the sidelines. Embedded support reflects the reality of how women experience their health in an interconnected and overlapping way.